This cross-sectional study investigated for the first time the choice of OP and HP, selection differences under different BMI, and the relevant basis of rehabilitation practitioners in the Chinese Mainland through online questionnaires. It was found that the vast majority of rehabilitation practitioners surveyed (96.74%) believed that spinal posture re-education is very important in clinical practice, which is consistent with the suggestion of the Association of Physiotherapists [
17]. Although posture re-education may play a role in managing spinal pain in some patients, there is no substantial evidence to show the specific posture that causes spinal pain. Perhaps because of “conforms to the natural alignment of the spine” or based on ergonomics and biomechanics considerations, most rehabilitation practitioners believe that the trunk upright lumbar lordosis posture in the SP and StP is the most optimal, while the lazy posture or the head-forward posture is a HP, which is consistent with previous research [
15].
However, general stereotyping of posture may be based more on clinical views than on experimental evidence. Roussouly et al. [
18] divided four sagittal shapes of the spine using X-ray images and found that the change in the pelvic inclination angle affects the global spinal alignment, while the pelvic inclination angle can change with posture. Muyor et al. [
19] compared a motion capture system with an X-ray radiograph image and observed that there was high consistency (ICC = 0.90) in evaluating the sagittal force line of the spine. Mousavi et al. [
20] tested the reliability of repeated measurements with Vicon and showed excellent consistency in the pelvic tilt angle, lumbar lordosis, and thoracic kyphosis. Therefore, as a harmless, repeatable, and accurate assessment tool, Vicon can quantify various posture angles.
4.1. Clinical Significance of Spinal Angle
Kendall et al. [
3] and Woodhull et al. [
2] believe that the optimal StP involves a neutral pelvic position, mild lumbar kyphosis, and head in a balanced position, but no specific angle value was given; therefore, there is still much controversy about the optimal StP. Subsequent researchers [
6,
8,
9,
21] also studied the alignment arrangement of postures; only Korakakis et al. [
15] used Vicon to quantitatively measure the angles of different postures, and the results were similar to those of this study; however, because the model in that study was a woman, there was still some deviation in the specific angle.
The increase in pelvic inclination angle may result in increased lumbar curvature or downward movement of curved vertices and lumbar curvature flattening [
18]. Therefore, this study mainly used PA combined with LSA to describe the positions of the pelvis and lumbar vertebrae. PA represents the degree of pelvic tilt in the sagittal plane. The pelvic anteversion angle was defined as positive, and the posterior tilt angle was defined as negative. Lumbar lordosis was defined as positive and kyphosis as negative to prevent two different lumbar angle changes, combined with LSA to describe the lumbar lordosis angle. The combination of these two angles can show the curve of the entire pelvis and lumbar spine. Concurrently, CTA was used to describe the degree of the head forward, which is an important method to evaluate the upright torso [
2]. The smaller the CTA value, the more serious the head protrusion.
Table 2 and
Table 3 show the other angle differences, which are no longer described in this study.
Upright lordotic postures are considered optimal despite the lack of strong evidence that any specific posture is linked to better health outcomes. While postural re-education may play a role in managing spinal pain in some patients, awareness of widespread and stereotypical beliefs regarding OP may be helpful in clinical assessment and management. For overweight or obese people, the observation of the physiotherapists may be incorrect, so further physical examination or quantitative equipment is needed for posture evaluation.
4.2. The Choice of Optimal Standing and Sitting Postures in Different Body Mass Index
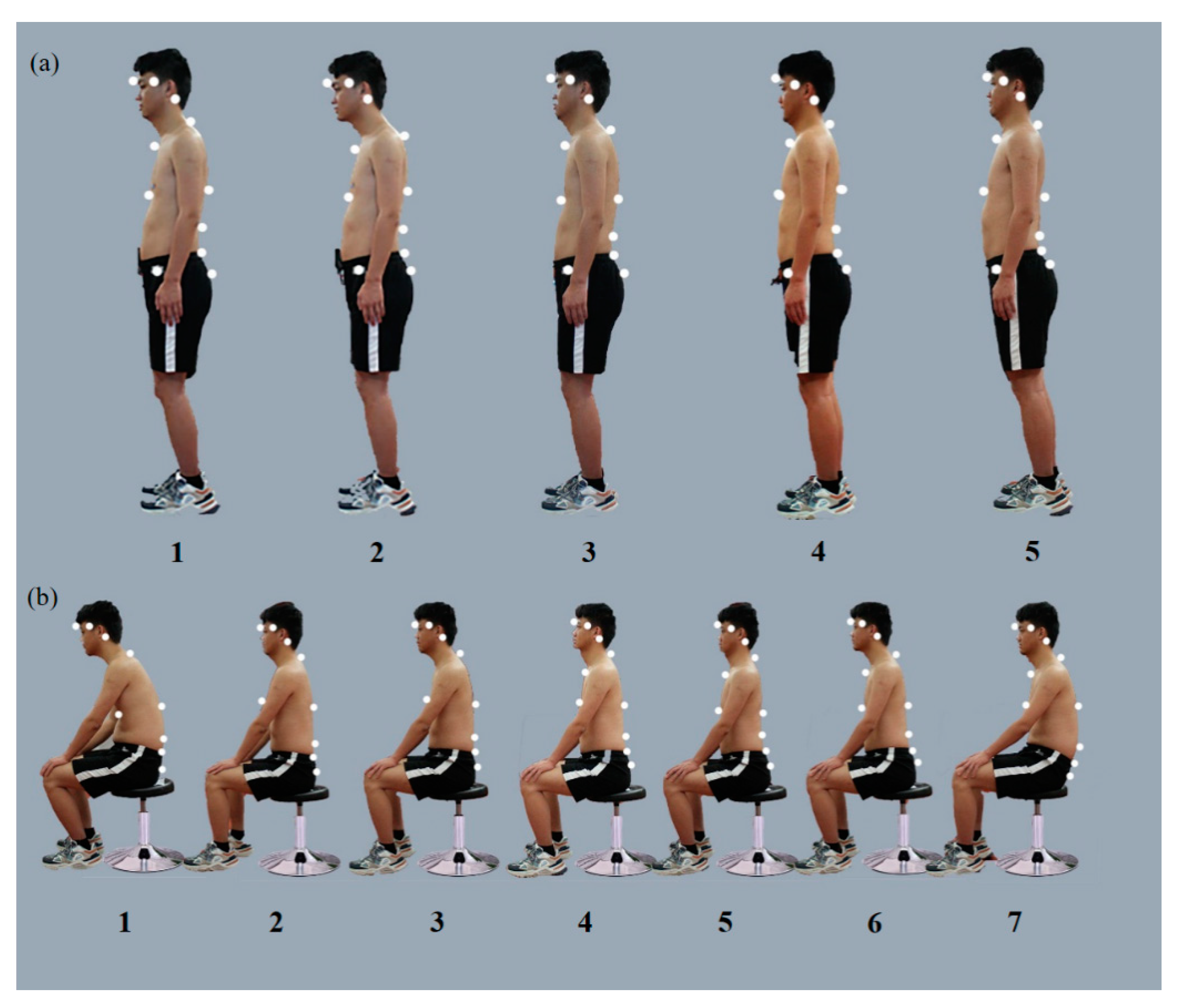
In this study, the rehabilitation practitioners were asked to observe photographs of different postures to choose OP and HP. Thus, the observation process of the therapist in daily work was imitated. The results showed that most of the rehabilitation practitioners considered sitting posture 1-4 (CTA = 159.98°, LSA = 163.22°, PA = −10.52°), 1-5 (CTA = 155.96°, LSA = 163.22°, PA = −25.9°); and 2-4 (CTA = 159.02°, LSA = 168.99°, PA = 3.08°) of lumbar lordosis with the trunk upright as the OP, while 25.72% chose sitting posture 1-2 (CTA = 157.14°, LSA = 156.36°, PA = −1.40°) with the trunk upright and flat back.
However, some studies have pointed out that sitting positions 4 and 5 of lumbar lordosis activate more trunk muscles than the flat-back posture 2 [
17,
22,
23], which may cause neck pain [
24] and low back pain [
25]. The long-term maintenance of the lumbar lordosis sitting posture is also questioned, as this state may exceed the bearing capacity of the paraspinal muscles [
22], resulting in greater fatigue, pain, and discomfort in the neck and waist [
26]. However, in a previous study [
15], physiotherapists still chose the lumbar lordosis sitting posture in the vast majority (95.7%), which is consistent with our study.
Most of the rehabilitation practitioners chose standing posture 1-4 (CTA = 157.92°, LSA = 148.32°, PA = 9.93°), 2-3 (CTA = 162.74°, LSA = 153.83°, PA = 19.38°), and 2-5 (CTA = 165.73°, LSA = 153.51°, PA = 18.63°) as the optimal StP, mostly based on biomechanical models, such as vertical alignment of gravity lines [
5,
6], or “best” sagittal balance [
18]. Roussouly et al. [
18] recorded the changes in the sagittal plane of the standing spine through a prospective radiological study and divided the spinal curve into four categories:
Lower lumbar segmental kyphosis and kyphosis in the thoracolumbar joint and thoracic vertebrae;
Flatter spine, less thoracic kyphosis, and lumbar kyphosis;
The inflection point of thoracic kyphosis, lumbar kyphosis at the thoracolumbar junction, and the peak of lumbar kyphosis at L4;
Both the lumbar vertebrae and thoracolumbar joints are kyphotic.
Although the authors hypothesized that the type 3 spine is the “most balanced” posture, the correlation between spinal morphology and symptoms is unclear.
Some studies have proposed the use of a lumbar “neutral position” (defined as in the middle position and/or mild kyphosis) to relieve passive tissue tension in the terminal position, as to reduce potential pain [
27] and facilitate the critical postural stabilizer muscle [
22] and reduce the incidence of low back pain [
28]. However, the neutral position is affected by age [
29], lumbar mobility [
17], and other factors. There is no consensus on whether the neutral position is actually upright or flexion.
4.3. The Choice of Harmful SP and StP with Different BMI
For the harmful SP, approximately 90% of the rehabilitation practitioners chose SP 1 of kyphosis and forward head 1-1 (CTA = 137.21°, LSA = 174.53°, PA = −14.39°) and 2-1 (CTA = 135.90°, LSA = 165.99°, PA = −12.80°). Moreover, 83.7% and 92.39% of the rehabilitation practitioners chose StP 1-2 (CTA = 155.52°, LSA = 153.69°, PA = 9.59°) and 2-2 (CTA = 157.49°, LSA = 154.76°, PA = 15.88°), respectively. However, some rehabilitation practitioners selected SPs 1-4 (12.32%) and 1-5 (12.68%) as HPs, although nearly half of the practitioners chose these two postures as OP, which is also consistent with the previous discussion on OP. It is believed that SP 4 and 5 may activate more muscles and cause spinal pain.
The choice of HP may reflect the long-standing view that flexion posture in the sitting position is related to increased intervertebral disc pressure [
12,
13], intervertebral disc creeps [
14], and intervertebral disc degeneration. Nevertheless, the head protrusion position increases the load on the neck and fatigue of the neck extensor [
16], which may cause neck pain [
30]. Moreover, excessive lumbar kyphosis can excessively activate the paraspinal muscles [
17,
22,
23], increasing facet joint pressure [
18] and resulting in low back pain.
4.4. The Influence of Subspecialty on Posture-Related Choice
Rehabilitation practitioners generally believe that posture education is “quite” and “very” important in clinical practice. In all subspecialties, musculoskeletal, sports injuries, and children-oriented PT are more likely to evaluate the patient’s posture frequently, which may be due to the subprofessional’s need to assess whether the systemic or spinal axial symptoms of patients are related to a specific posture [
15]. However, musculoskeletal and sports injury PTs are more inclined toward training posture, which may be related to the attributes of patients; these patients have no neurological abnormalities, most of them experience chronic pain, and they are often treated with static and dynamic postural habits [
8,
31].
Rehabilitation practitioners have a relatively uniform concept of HP; however, for optimal SP, professionals with younger and higher workplace levels were more inclined to choose sitting postures 4 and 5. This may be because the quality of medical care is proportional to the level of hospitals in China, and young practitioners are trained well by instructors in senior hospitals, resulting in a unified perception, or by associations of therapists [
17].
Overall, rehabilitation practitioners tend to believe that OPs include an upright torso, mild lumbar kyphosis, and relative relaxation of the thoracic vertebrae based on the natural morphology of the spine and biomechanical principles and head retraction rather than kyphosis [
23], though the “perfect posture” is a rare standard. Moreover, no specific normal posture or OP exists, and maintaining the same posture for a long time, no matter how ideal it is, will cause symptoms. Frequent changes in posture are required. Relatively, the concept of HP is the same, such as head protrusion and spinal flexion are obvious signs. Healthy people habitually assume a flexion spine posture in their work and life. Teaching patients to avoid such postures may be beneficial to some extent. Therefore, for clinical rehabilitation practitioners, it may be easier to unify and implement posture re-education to teach patients what constitutes a HP and to how to avoid it as well as to recommend frequent changes in posture.
4.5. Limitation
This study was limited to SPs and StPs of the static sagittal plane, and only a few spinal configurations were available to choose from, which could not include all postures. Therefore, reflecting on the dynamic changes in daily posture is difficult. The models used in the study were young men; however, differences in sex and age can also affect posture judgment. The rehabilitation practitioners involved in the survey were also young and had a low level of education and professional titles, which may have also resulted in some differences in the results. In addition, considering the small angle differences between some positions and changes in skin tissue adhesion and the surface of markers, unknown measurement errors may have occurred. For the quantification of sagittal spinal posture, CTA, LSA, and PA are more sensitive for identifying optimal and harmful spinal morphology, which can be further studied, providing a basis for follow-up research and development of simplified equipment. Further exploration is needed to assess whether postural feedback from wearable devices will affect the incidence and persistence of spinal pain.

 ,
, 
{kind=link}
{kind=link}
{kind=link}


